INTERNSHIP PORTFOLIO NAVYA SRI PABBA ROLLNO :76
HELLO, I AM NAVYASRI PABBA, INTERN 2k18 BATCH.
I AM HERE TO SHARE MY INTERNSHIP JOURNEY IN THE MEDICINE DEPARTMENT. FIRST AND FOREMOST, I WOULD LIKE TO EXPRESS MY GRATITUDE TO OUR RESPECTED HEAD OF DEPARTMENT (HOD), FACULTY, AND POST-GRADUATE SIRS AND MADAMS WHO GUIDED ME AT EVERY STEP, ENABLING ME TO SUCCESSFULLY COMPLETE MY INTERNSHIP DESPITE ENCOUNTERING NUMEROUS CHALLENGES.
MY JOURNEY INTO MEDICINE COMMENCED DURING MY 5TH SEMESTER, BUT MY GENUINE INTEREST IN THE FIELD DEVELOPED DURING MY SCHOOL YEARS. THE ART OF CRAFTING BLOGS HAS SIGNIFICANTLY ENRICHED MY LEARNING EXPERIENCE. IN THE 5TH SEMESTER, WITNESSING A PATIENT IN THE MEDICINE ICU EXPERIENCING SHORTNESS OF BREATH TRIGGERED A QUESTION IN MY MIND ABOUT THE CAUSE. INITIALLY, I CONSIDERED ACUTE LUNG INJURY, BUT WITH GUIDANCE FROM OUR RESPECTED MEDICINE HOD AND OTHER FACULTY MEMBERS, I DELVED INTO UNDERSTANDING THE CASE SCENARIO. I DOCUMENTED THIS JOURNEY IN A BLOG, ULTIMATELY CONCLUDING THAT THE ROOT CAUSE OF THE PATIENT'S SHORTNESS OF BREATH WAS RIGHT HEART FAILURE.
THESE ARE THE OTHER BLOGS WHICH I HAVE MADE IN MY UG LIFE
1.PERSONAL DISTUBANCES IN A PATIENT LIFE LANDED UP HIM INTO ALCOHOL WITHDRAWAL
2.57 YEAR OLD M WITH BILATERAL PEDAL EDEMA AND DECREASED URINE OUTPUT
3.67 YEAR OLD MALE WITH BODY PAINS AND FEVER
4.70 Y OLD FEMALE WITH FEVER AND CHILLS
NOW BEGINS MY INTERNSHIP LIFE, FILLED WITH EXCITEMENT AND ENTHUSIASM TO DEEPEN MY UNDERSTANDING OF MEDICINE PRACTICALLY.

MY FIRST INTERACTION WAS WITH


I PRESENTED THE FOLLOWING CASE OF ALTERED SENSORIUM ON 12/10/2023
CASE 1-
A 73-YEAR-OLD FEMALE, FROM WHOM I LEARNED THAT HYPERTENSIVE URGENCY COULD LEAD TO BRAIN INFARCTION, EVIDENT IN HER LACUNAR INFARCT IN THE FRONTAL LOBE.
WHILE IN THE CASUALTY, HER ATTENDER BROUGHT HER IN A DROWSY STATE, NOTING BEHAVIORAL CHANGES AND URINARY INCONTINENCE HOURS PRIOR. FROM HER ADMISSION TO DISCHARGE, I OBSERVED EVERY ASPECT OF HER TREATMENT AND WITNESSED REMARKABLE IMPROVEMENT.
THIS EXPERIENCE ILLUSTRATED THAT OUR RESPECTED HOD SIR AND FACULTY, WITH THEIR KNOWLEDGE, PLAYED A PIVOTAL ROLE IN GIVING THIS WOMAN A SECOND LIFE. IT IGNITED A STRONG INTEREST IN ME TO PURSUE MEDICINE AS MY DREAM SPECIALTY IN RESIDENCY.
BLOG LINK
WATSAPP PAJR LINK
THE FOLLOWING IS THE CONVERSATION BETWEEN ME ; OUR RESPECTED HOD AND FACULTY MEMBERS WHICH HELPED US TO TREAT PATIENT
OSCE
[06/10, 2:52 pm] Rakesh Biswas Sir: When and where admitted?
[07/10, 9:32 am] Rakesh Biswas Sir: 👆
[07/10, 11:02 am] Navya Sri. Pabba: Sir ICU bed no. 1 sir
[07/10, 11:02 am] Navya Sri. Pabba: On 5/10/23
[07/10, 11:03 am] Navya Sri. Pabba: I will update the pajr after assigning interns sir
[07/10, 3:29 pm] Rakesh Biswas Sir: Please share her plotted fever chart and check for meningeal signs!
Can her fever and altered sensorium be due to meningitis!
Was she on any antibiotics?
[07/10, 3:35 pm] Navya Sri. Pabba: Sir i will share
[07/10, 3:38 pm] Rakesh Biswas Sir: Well done history in the description box! Get ready to present her on 19th October along with Haripriya.
So if a patient has febrile encephalopathy like her and there's no meningitis on CSF examination, then one can even think of other sepsis causing encephalopathy and sometimes even meningism which as per your findings the patient doesn't have.
Can get our PGs or EMD PGs or Anesthesia PGs to do her CSF and then you can also do the next one
[07/10, 4:50 pm] Navya Sri. Pabba: Ok sir
CASE 2-
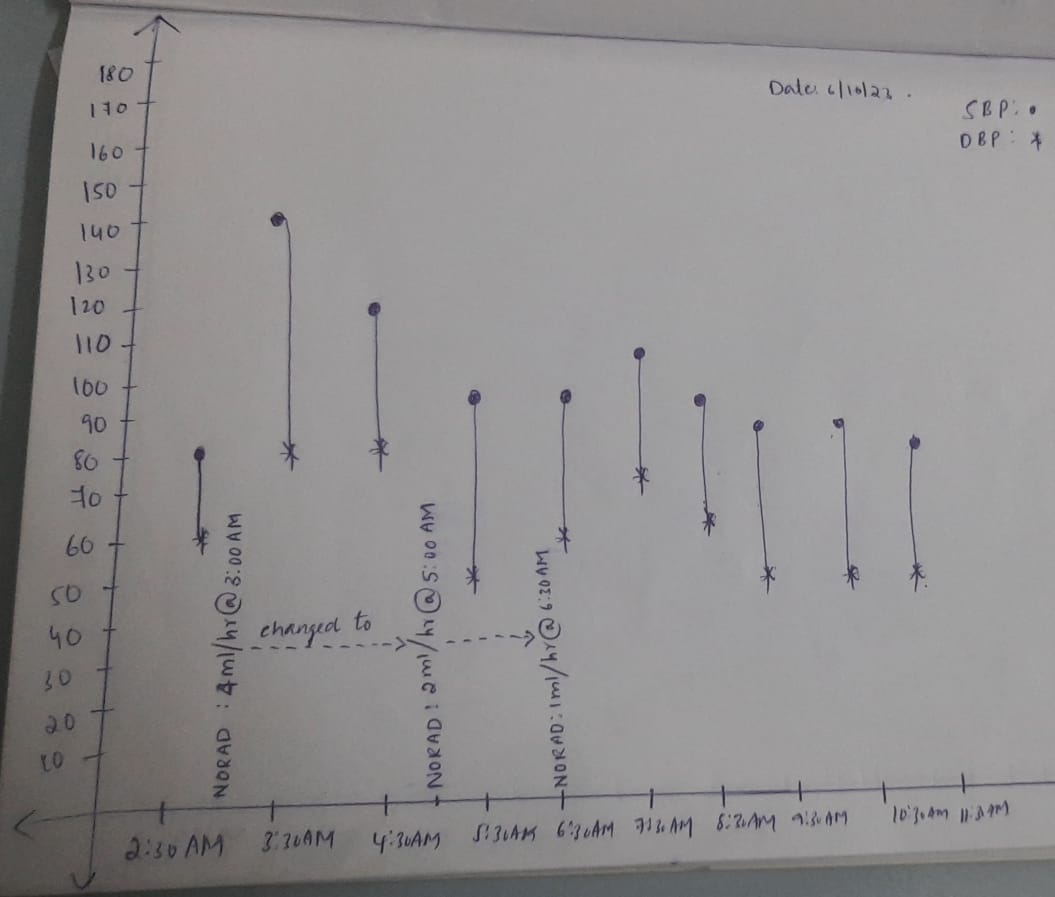
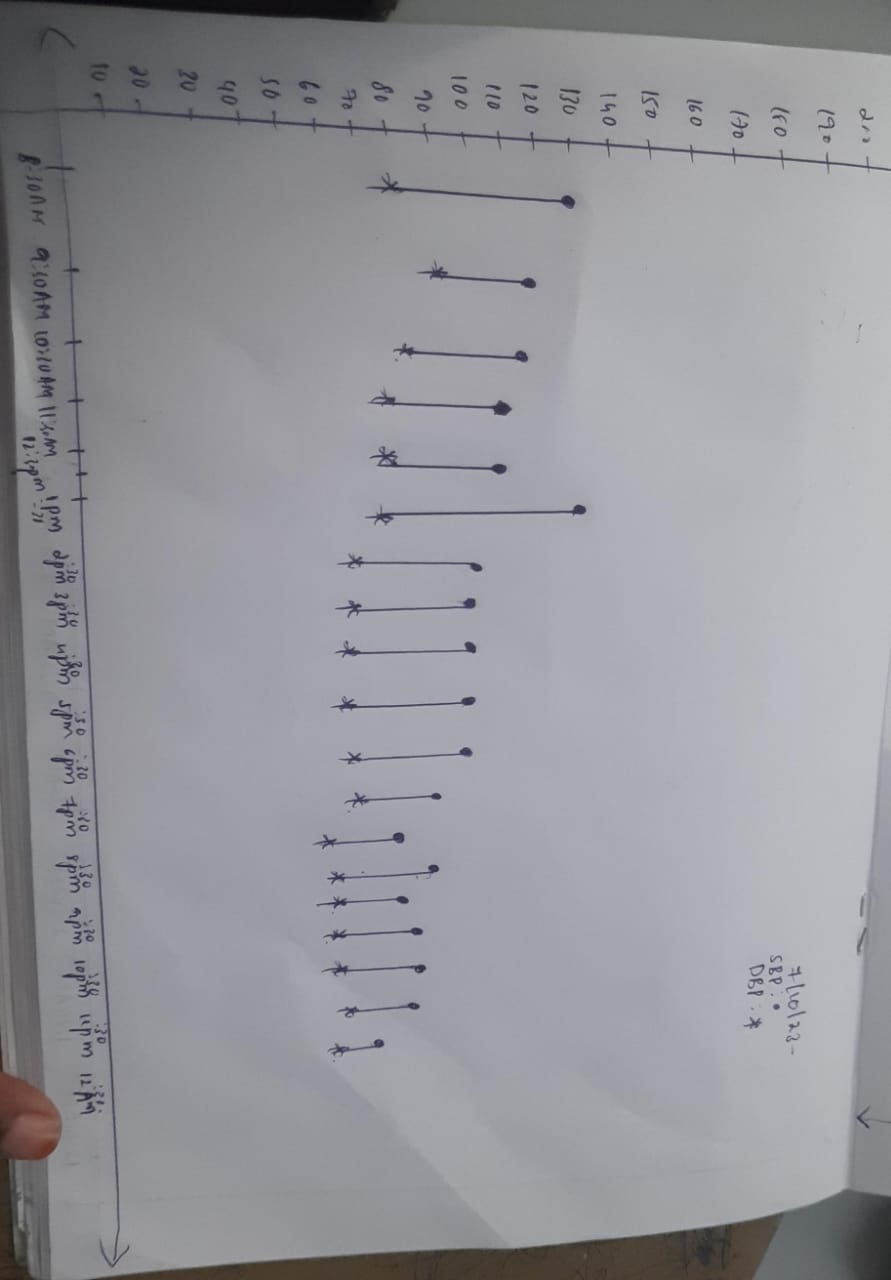
A 74-YEAR-OLD MALE PATIENT ARRIVED AT THE CASUALTY WITH GIDDINESS. I WAS EAGER TO SEE HOW HE COULD BE BROUGHT BACK TO NORMAL AND WHICH INTERVENTIONS WOULD ACHIEVE THAT.
I MONITORED HIS BLOOD PRESSURE HOURLY FOR A WEEK, ENABLING ADJUSTMENTS IN INOTROPIC SUPPORT. MY DEDICATION PAID OFF, AND THE PATIENT AND ATTENDANT WERE TRULY HAPPY.




WE FACILITATED DRESSING FOR THE PATIENT, AND DESPITE MY SURGICAL INTERNSHIP, I ASSISTED A SURGERY RESIDENT IN MANAGING THE CELLULITIS. THE INTERNSHIP PROVIDED SUFFICIENT INSIGHT TO TREAT A MEDICINE PATIENT WITH CONCURRENT SURGICAL ISSUES.
I AM GRATEFUL TO MY HOD FOR GRANTING ME THIS OPPORTUNITY TO LEARN MEDICINE AND SURGERY SIMULTANEOUSLY.
WATSAPP PAJR LINK
OSCE-
[06/10, 2:53 pm] Rakesh Biswas Sir: ICU 4?
[06/10, 2:53 pm] Navya Sri. Pabba: Yes sir
[06/10, 4:14 pm] Rakesh Biswas Sir: Share his BP charts right from his first BP asap
[06/10, 4:15 pm] Navya Sri. Pabba: Ok sir
[06/10, 4:16 pm] Rakesh Biswas Sir: Make me Admin
[06/10, 4:16 pm] Navya Sri. Pabba: Ok sir
[06/10, 4:26 pm] Rakesh Biswas Sir: Interventions such as norad during the times mentioned along with drip rate
[06/10, 4:28 pm] Navya Sri. Pabba: I will update sir
[06/10, 4:52 pm] Navya Sri. Pabba: Norad is given sir
[06/10, 4:54 pm] Rakesh Biswas Sir: Thanks
[07/10, 8:55 am] Navya Sri. Pabba: Watery discharge from lower half of left leg since yesterday 6 pm
[07/10, 9:11 am] Rakesh Biswas Sir: How long would it take to reach tachyphylaxis for noradrenaline beyond which time it becomes ineffective? Can you discuss this with our Pharmacology PG and add her here?
[07/10, 9:13 am] Navya Sri. Pabba: Ok sir
[07/10, 9:15 am] Rakesh Biswas Sir: For all these SpO2s what's the FiO2?
[07/10, 9:17 am] Rakesh Biswas Sir: Always share this graphical timeline for every inpatient (and if possible for our outpatients with regular follow up) regardless of their fever status as this is also a quick graphical timeline of the patient's soap and not just the fever 👇
http://durgakrishna09.blogspot.com/2023/08/graphical-patient-timeline-in-soap.html
[07/10, 9:17 am] Navya Sri. Pabba: We didn't put him on CPAP sir
[07/10, 9:18 am] Navya Sri. Pabba: Ok sir
[07/10, 9:21 am] Rakesh Biswas Sir: What is the FiO2 you are breathing right now?
We want to know if the SpO2 values you shared were on room air (FiO2 of 0.21) or higher!!
[07/10, 9:22 am] Navya Sri. Pabba: Room Air sir
[07/10, 9:22 am] Navya Sri. Pabba: 21%
[07/10, 9:22 am] Rakesh Biswas Sir: Sugar values?
[07/10, 9:22 am] Navya Sri. Pabba: Yes sir I am plotting the graph sir
[07/10, 9:23 am] Rakesh Biswas Sir: In the graph soap mention all objective variables for that day including for example BP, sugar, etc and the interventions used for each
[07/10, 9:24 am] Navya Sri. Pabba: Ok sir
[07/10, 9:28 am] Navya Sri. Pabba: Sir I contacted pharma Pg maam
[07/10, 9:34 am] Navya Sri. Pabba: Sir I will shortly update the BP Charting and GRBS IN Graphical representation
[07/10, 9:37 am] Rakesh Biswas Sir: You were supposed to tag every current inpatient to the current intern responsible and share it in the ward group!
Please do that first and share it asap
I also want you to select one of our current patients of altered sensorium to be presented in the upcoming Thursday clinical meeting on 19/10 asap
[07/10, 9:38 am] Rakesh Biswas Sir: 👆Already shared
[07/10, 9:38 am] Navya Sri. Pabba: @10:00pm norad was changed to
5 ml/hr sir
[07/10, 9:38 am] Navya Sri. Pabba: This I updated sir
[07/10, 9:38 am] Rakesh Biswas Sir: Yesterday?
[07/10, 9:39 am] Navya Sri. Pabba: Yes sir yesterday 10 :00 pm
[07/10, 9:39 am] Rakesh Biswas Sir: What will be it's effect on the expected tachyphylaxis?
[07/10, 9:39 am] Rakesh Biswas Sir: 👆
[07/10, 9:41 am] Navya Sri. Pabba: Yes sir I will tag them sir
[07/10, 5:04 pm] Rakesh Biswas Sir: You need to review the literature around blisters heralding spontaneous cellulitis in Diabetes
[07/10, 5:12 pm] Navya Sri. Pabba: Ok sir
[09/10, 1:01 pm] Rakesh Biswas Sir: How's he today soap?
[09/10, 1:27 pm] Navya Sri. Pabba: 09/10/2023
Ward :AMC
Unit : 4
DOA : 05/10/2023
S : No new complaints
O:
Patient is conscious coherent and cooperative
Pallor ,icterus
clubbing, cyanosis, lymphadenopathy, oedema.- Absent
Vitals :
BP- 100/60mmHg
PR -78bpm
RR-16 cpm
Temperature -98.3 F
Grbs:136mg/dl
CVS: S1,S2 heard , no murmurs.
RS: BAE, NVBS, no added sounds.
P/A: soft non tender; no organomegaly
A: SEPTIC SHOCK WITH AKI LEFT LOWER LINB CELLULITIS
K/C/O HTN SINCE 15 YEARS
T2 DM SINCE 15 YEARS
P:
1.IV FLUIDS@ 100/HR
2.INJ PAN 40 MG IV / BD
3. INJ NEOMAL 1GM / IV / SOS
4.INJ ZOFER 4MG IV/ SOS
5.NJ HAI S/C TID BEFORE MEALS
[09/10, 2:19 pm] Rakesh Biswas Sir: BP chart since admission?
Also share the fever chart asap to allow us to understand at a glance what we have done and found differently each day since 5/10/23 asap
[09/10, 2:28 pm] Navya Sri. Pabba: Ok sir
[09/10, 2:40 pm] Rakesh Biswas Sir: Please share updates on your altered sensorium patient that you are going to present on 19/10
[09/10, 2:46 pm] Navya Sri. Pabba: Ok sir
[09/10, 4:03 pm] Rakesh Biswas Sir: No interventions here?
[09/10, 4:03 pm] Rakesh Biswas Sir: What time were the inotropic interventions stopped?
[09/10, 4:04 pm] Navya Sri. Pabba: Norad was discontinued on 7/10/22
@ 7 pm sir
[09/10, 4:04 pm] Navya Sri. Pabba: 7/10/23*
[09/10, 4:07 pm] Rakesh Biswas Sir: 👆As per your chart it appears to have been stopped at 10:10 PM on 6/10?
[09/10, 4:10 pm] Navya Sri. Pabba: It is continued sir upto 7pm on 7/10/2023
Case 3
40M PAIN ABDOMEN, ascites, oliguria 2 DAYS Congenital Neural tube defect
BLOG LINK-

WATSAPP PAJR LINK-
OSCE-
[27/10, 7:55 pm] Rakesh Biswas Sir: Well done. Please YouTube this and share the link. Also let me know asap the cell type and cell count
[27/10, 7:58 pm] Rakesh Biswas Sir: 👆Reason for raised alkaline phosphatase?
Intestine or bone?
[27/10, 8:01 pm] Rakesh Biswas Sir: Mystery solved with a proper history of present illness dating back to his childhood as shared in caps lock below by @Navya Sri. Pabba :
HE HAD A SWELLING IN MIDLINE LOWER LUMBAR REGION WHICH IS ABOUT 2×2 CM SINCE BIRTH
AT THE AGE OF 7 YEARS HE GOT OPERATED ON THAT SWELLING AND SINCE THEN HE DEVELOPED NEUROGENIC BLADDER FOR WHICH HE WAS CONSERVATIVELY MANAGED WITH FEW MEDICATION
K/C/O CKD SINCE 10 YEARS ON CONSERVATIVE MANAGEMENT AND ON FOLEYS
K/C/O HTN SINCE 1 YEAR IT IS DIAGNOSED ON A ROUTINE EXAMINATION AS A PART OF TREATMENT TO CKD
H/O BACKPAIN SINCE 5YEARS
More history needed about his quadriparesis subjectivity!!
[27/10, 8:05 pm] Rakesh Biswas Sir: 👆How much is the RVSP written here?
[27/10, 8:11 pm] Navya Sri. Pabba: 75 mm Hg sir
[27/10, 8:12 pm] Navya Sri. Pabba: I will update sir
[27/10, 8:12 pm] Navya Sri. Pabba: Ok sir
[27/10, 8:14 pm] Rakesh Biswas Sir: And what is the severity of pulmonary hypertension written as?
[27/10, 8:39 pm] Navya Sri. Pabba: As No PAH sir
[27/10, 8:39 pm] Rakesh Biswas Sir: How do we explain this discrepancy?
[27/10, 8:46 pm] Navya Sri. Pabba: Sir it is interpretation error
I will confirm and I will update it sir
[28/10, 10:22 am] Haripriya Maam Medicine Pg 2 Yr: Todays Update
@Navya Sri. Pabba
[28/10, 10:50 am] Haripriya Maam Medicine Pg 2 Yr: U didn’t mention about the lowerlimbs deformity @Navya Sri. Pabba
[28/10, 10:54 am] Navya Sri. Pabba: Maam he is having valgus deformity since 3 years
[28/10, 10:54 am] Haripriya Maam Medicine Pg 2 Yr: And also mention about how he was diagnosed with CKD
[28/10, 10:54 am] Navya Sri. Pabba: I will update sir
[28/10, 10:55 am] Navya Sri. Pabba: He had left side back pain 10 years back and he went to hospital and he is diagnosed with ckd maam
[28/10, 10:56 am] Haripriya Maam Medicine Pg 2 Yr: Yes
Mention that,and also mention how it started and progressed,Is that intervened in any other way for his deformity,does that deformity caused any disturbance in his work/daily activities
and is there any associated sensory symptoms and motor symptoms (like power disturbances)
[28/10, 11:01 am] Haripriya Maam Medicine Pg 2 Yr: And in the dp
You can add his lowerlimbs image also
[30/10, 12:57 pm] Navya Sri. Pabba: He had valgus deformity since 10 years maam and it doesn't cause any disturbance to do his daily activities
No associated Sensory symptoms or motor symptoms
[30/10, 2:17 pm] Rakesh Biswas Sir: Thanks @Navya Sri. Pabba
Ascites showing a cell count in 7000s with 100% looks more like secondary rather than spontaneous peritonitis!
Is the peritonitis due to his associated pancreatitis?
Is the history suggestive of pancreatitis?
[30/10, 2:19 pm] Rakesh Biswas Sir: Lots of BP medications!
Can you share the BP charts post admission? Also mention there the interventions and time they were taken and the time the BP was taken
[30/10, 2:23 pm] Rakesh Biswas Sir: The USG does show moderate hydro uretero nephrosis indicating a possible etiology for his CKD in neurogenic bladder
Would have been happier if we could see the USG video findings!
[30/10, 2:27 pm] Rakesh Biswas Sir: History sketchy does hint at pancreatitis although USG suggests he could be having a chronic liver disease too! What could be the reason for that? Viral serology done?
Also the USG shows a normal body of pancreas but then not sure if they saw it well and also do we need a CT abdomen to chase the pancreas further with tax payer's money (Arogyashree)? Is it worth chasing further?
[30/10, 2:29 pm] Rakesh Biswas Sir: Low grade fever spikes with secondary peritonitis is still difficult to explain with pancreatitis! We are still missing something although his neurological problem which was confusing on Friday was sorted on Friday itself by @Navya Sri. Pabba
[30/10, 2:53 pm] Deepika Maam Kims: Problem presentation -
Fall in haemoglobin ? 7--> 5.4
Ascitis ( low SAAG,high protein)
? Bacterial peritonitis?( secondary/ spontaneous)( sepsis)
Pancreatitis??
Ckd 2° to ? Reflux nephropathy( neurogenic bladder)
Hypertension
Spastic paresis
[30/10, 2:56 pm] Rakesh Biswas Sir: Answered all above except the first one!
When was it 7 and when was it 5.4?
[30/10, 2:56 pm] Deepika Maam Kims: Sir could there be possibility of any active bleed Considering the fall in Hb?
[30/10, 2:57 pm] Rakesh Biswas Sir: Isn't neurogenic bladder adequate for CKD etiology? How does one confirm Vesico ureteral reflux?
[30/10, 2:57 pm] Rakesh Biswas Sir: Between which days?
[30/10, 3:01 pm] Deepika Maam Kims: Reflux nephropathy can be direct consequence of VUR or any conditions causing increased pressure in bladder ( Bladder outlet obstruction, neurogenic bladder etc ) sir
[30/10, 3:05 pm] Deepika Maam Kims: 26th night (11pm)Hb - 7
28th - 5.3 sir
[30/10, 3:08 pm] Rakesh Biswas Sir: Share the BP charts in between 26-28
If he bled in between it may have reflected in her BP too although checking his postural fall would have been more useful
[30/10, 3:10 pm] Rakesh Biswas Sir: So when a patient develops hydroureteronephrosis from neurogenic bladder how commonly is it accompanied by Vesico ureteral reflux?
[30/10, 3:11 pm] Rakesh Biswas Sir: BP charts between 26-28
[31/10, 12:22 pm] Navya Sri. Pabba: 31/10/2023
Ward :AMC
Unit : 4
DOA : 26/10/2023
S :
PAIN ABDOMEN DECREASED
FLATUS PASSED
STOOLS- NOT PASSED
O:
Patient is conscious coherent and cooperative
Pallor ,icterus
clubbing, cyanosis, lymphadenopathy, oedema.- Absent
Vitals :
Temperature -96.8F
BP- 130/80mmHg
PR -102 bpm
RR-20 cpm
Grbs:137mg/dl
SPO2- 96 ON RA
I/O- 1350/650ml
CVS: S1,S2 heard , no murmurs.
RS: BAE+NVBS heard ,no added sounds.
P/A: Soft ; tenderness present in epigastric region, Bowel sounds+
CNS -
LEVEL OF CONSCIOUSNESS - CONSCIOUS
SPEECH - NORMAL
MENINGEAL SIGNS- ABSENT
CRANIAL NERVES- NORMAL
MOTOR SYSTEM- RT LT
TONE UL N N
LL N N
SENSORY SYTEM - NORMAL
GLASGOW SCALE- EVM 15/15
POWER RT LT
UL 3/5 3/5
LL 3/5 3/5
REFLEXES RT LT
BICEPS +3. +3
TRICEPS. +3. +3
KNEE REFLEX +3. +3
SUPINATOR +2 +2
ANKLE JERK +3 +3
PLANTAR REFLEX Flexor B/L
CEREBELLAR SIGNS- NORMAL
P:
1.FLUID RESTRICTION LESS THAN
1.5 L/DAY
2.SALT RESTRICTION LESS THAN
2 G /DAY
3.INJ PAN 40 MG IV/OD
4.INJ ZOFER 1G IV /SOS
5.INJ LASIX 40MG IV/BD
6.INJ BUSCOPAN 1 AMP /IM/SOS
7.INJ EPO 4000 IV /SC/ ONCE WEEKLY
8.TAB.NODOSIS 500 MG PO/TID
9.TAB OROFER XT PO/OD
10.TAB.SHELCAL - PO/OD
11.TAB ARKAMINE 0.1MG /PO/TID
12.TAB MINIPRESS XL 2.5 MG PO/OD
13 TAB SEVELEMAR 400MG /PO/BD
14.SYP POTKLOR 10ML IN GLASS OF WATER PO/TID
[01/11, 10:10 am] Haripriya Maam Medicine Pg 2 Yr: !!!
[01/11, 10:11 am] Haripriya Maam Medicine Pg 2 Yr: !!!!
[01/11, 10:11 am] Haripriya Maam Medicine Pg 2 Yr: Which is correct 3 or 10 years @Navya Sri. Pabba
[01/11, 10:12 am] Navya Sri. Pabba: 10 years MAAM
CASE 4
BLOG LINK-
WATSAPP PAJR -
OSCE -
[13/10, 2:38 pm] Rakesh Biswas Sir: Left axis with poor progression of r wave
[13/10, 2:40 pm] Rakesh Biswas Sir: Well done data capture
Metabolic syndrome CAD CCF CKD
A very common NCD story
[14/10, 9:17 am] Navya Sri. Pabba: 14/10/2023
Ward :ICU
Unit : 4
DOA : 12/10/2023
S : No fever spikes
O:
Patient is conscious coherent and cooperative
Pallor ,icterus
clubbing, cyanosis, lymphadenopathy, oedema.- Absent
Vitals :
Temperature -98.9 F
BP- 130/80mmHg
PR -54bpm
RR-16 cpm
Grbs:124 mg/dl
CVS: S1,S2 heard , no murmurs.
RS: BAE, NVBS, no added sounds.
P/A: soft non tender; no organomegaly
CNS - Normal
A: DILATED CARDIOMYOPATHY WITH
EF - 54% SECONDARY TO ALCOHOL INTAKE WITH AKI ON CKD WITH GRADE II BED SORE
P:
1.FLUID RESTRICTION LESS THAN
1 L/DAY
2.SALT RESTRICTION LESS THAN
2 TO 3 G /DAY
3.FREQUENT POSITION CHANGE
4.INJ LASIX 100 MG ( 10ML) + 40ML NS INFUSION @ 3ML/HR
5.INJ THIAMINE 1 AMP IN 100 ML NS IV/TID
6.TAB.SPIRANOLACTONE 25 MG PO/BD
[14/10, 9:20 am] Rakesh Biswas Sir: Fever chart daily soaps at a glance?
[14/10, 9:26 am] Navya Sri. Pabba: He is afebrile sir
[14/10, 9:27 am] Navya Sri. Pabba: I will update sir
[14/10, 9:35 am] Rakesh Biswas Sir: Yes that Chart is not just about fever but about the daily soaps at a glance
[14/10, 9:48 am] Navya Sri. Pabba: Ok sir
[14/10, 9:48 am] Navya Sri. Pabba: I will update sir
[14/10, 10:09 am] Rakesh Biswas Sir: Daily input output?
[14/10, 10:15 am] Navya Sri. Pabba: Updated sir
[14/10, 2:18 pm] Rakesh Biswas Sir: Why is he having polyuria inspite of fluid restriction with a negative fluid balance of 2 liters?
[14/10, 2:58 pm] Navya Sri. Pabba: Because he is on Lasix sir
[14/10, 2:59 pm] Navya Sri. Pabba: And he had anasarca on the
Day of presentation
[14/10, 3:00 pm] Navya Sri. Pabba: So by giving Lasix all the interstitial fluid is being excreted out sir
[16/10, 10:22 am] Rakesh Biswas Sir: Is 50 mg once daily spironolactone more rational than 25 mg twice daily as you have outlined?
[16/10, 5:02 pm] Dr. Lohith Varma Jampana: 2decho!
[16/10, 5:02 pm] Navya Sri. Pabba: Review 2d echo
[16/10, 5:02 pm] Navya Sri. Pabba: Yes sir
[16/10, 5:13 pm] Dr. Lohith Varma Jampana: Dilated cardiac chambers have reversed sir!
[16/10, 5:20 pm] Dr. Lohith Varma Jampana: Alcohol Abstinence was the cure?
[17/10, 10:17 am] Rakesh Biswas Sir: Or repeated therapeutic Echo?
[17/10, 10:20 am] Dr. Lohith Varma Jampana: 😅
[17/10, 10:30 am] Rakesh Biswas Sir: Where is it documented that the chambers have reduced in size?
Vamshi did his thesis on this and serial chest X-rays were useful to document regression
[17/10, 10:31 am] Rakesh Biswas Sir: Just stopping alcohol for 10 days in someone taking it for 20 years can improve many things in 20 days 👏👏
[17/10, 12:44 pm] Navya Sri. Pabba: 17/10/2023
Ward :ICU
Unit : 4
DOA : 12/10/2023
S : No fever spikes
O:
Patient is conscious coherent and cooperative
Pallor ,icterus
clubbing, cyanosis, lymphadenopathy, oedema.- Absent
Vitals :
Temperature -99.2F
BP- 110/70mmHg
PR -60bpm
RR-17 cpm
Grbs:133 mg/dl
I/O- 900ml/1200ml
CVS: S1,S2 heard , no murmurs.
RS: BAE, NVBS, no added sounds.
P/A: soft non tender; no organomegaly
CNS - Normal
A: DILATED CARDIOMYOPATHY WITH
EF - 54% SECONDARY TO ALCOHOL INTAKE WITH AKI ON CKD WITH GRADE II BED SORE WITH HYPOKALEMIA SECONDARY TO DIURETICS

P:
1.FLUID RESTRICTION LESS THAN
1 L/DAY
2.SALT RESTRICTION LESS THAN
2 TO 3 G /DAY
3.FREQUENT POSITION CHANGE
4.INJ LASIX 40MG IV/BD
5.INJ THIAMINE 1 AMP IN 100 ML NS
IV/TID
6.TAB.SPIRANOLACTONE 25 MG PO/BD
7.SYP.POTCHLOR 10ML PO/TID IN 1 GLASS WATER
8.TAB.NODOSIS 500 MG PO/BD
9.TAB PCM 650 MG PO/BD
[18/10, 10:47 am] Rakesh Biswas Sir: 60 M??
There was a much younger man in ICU bed 4 !!
The one with bilateral above knee amputation?
[18/10, 10:49 am] Navya Sri. Pabba: He shifted to AMC THIS MORNING SIR
[18/10, 10:51 am] Rakesh Biswas Sir: Oh is he the one we made to stand and walk?
[18/10, 10:51 am] Navya Sri. Pabba: Yes sir
Case 5
BLOG LINK-
WATSAPP PAJR LINK-

OSCE -
[27/10, 7:32 am] Navya Sri. Pabba: 27/10/2023
Ward :MMW
Unit : 4
DOA : 26/10/2023
S : No fever spikes
O:
Patient is conscious coherent and cooperative
Pallor ,icterus
clubbing, cyanosis, lymphadenopathy, oedema.- Absent
Vitals :
Temperature -98.5F
BP- 110/70mmHg
PR -76bpm
RR-16 cpm
SpO2- 98 on RA
CVS: S1,S2 heard , no murmurs.
RS: BAE, NVBS, no added sounds.
P/A: soft non tender; no organomegaly
CNS - Normal
A:VIRAL PYREXIA WITH RIGHT UPPER LOBE CONSOLIDATION
? PULMONARY TUBERCULOSIS
P:
1.TAB PCM 650 MG PO/TID
2.TAB MONTEK LC PO/BD
3.SYRUP- ASCORYL - D 10ML PO/TID
[28/10, 10:07 am] Navya Sri. Pabba: 28/10/2023
Ward :MMW
Unit : 4
DOA : 26/10/2023
S : No fever spikes
O:
Patient is conscious coherent and cooperative
Pallor ,icterus
clubbing, cyanosis, lymphadenopathy, oedema.- Absent
Vitals :
Temperature -98.3F
BP- 110/70mmHg
PR -91bpm
RR-17 cpm
SpO2- 98 on RA
CVS: S1,S2 heard , no murmurs.
RS: BAE, NVBS, no added sounds.
P/A: soft non tender; no organomegaly
CNS - Normal
A:VIRAL PYREXIA WITH RIGHT UPPER LOBE CONSOLIDATION
? PULMONARY TUBERCULOSIS
WITH RETROVIRAL DISEASE POSITIVE
P:
1.TAB PCM 650 MG PO/TID
2.TAB MONTEK LC PO/BD
3.SYRUP- ASCORYL - D 10ML PO/TID
[28/10, 11:29 am] Rakesh Biswas Sir: Could you take him to the ART center Nalgonda in our ambulance or community medicine bus? Please discuss with the medical superintendent
[28/10, 11:30 am] Rakesh Biswas Sir: And Dr Manasa
[30/10, 1:02 pm] Navya Sri. Pabba: He want to get treatment in his native place sir
And as CD4 count facility is not available here He is referred to NACO sir
[30/10, 3:01 pm] Rakesh Biswas Sir: Where is his native place?
We wanted you to go to Nalgonda NACO and see how the CD4 is done and what art he is started on!
Now we've missed that opportunity!
[30/10, 3:03 pm] Navya Sri. Pabba: Choutuppal sir
[30/10, 3:12 pm] Rakesh Biswas Sir: Where is their nearest NACO. Please keep in touch with them and update as to what happens
[30/10, 3:28 pm] Navya Sri. Pabba: Ok sir
[30/10, 3:28 pm] Navya Sri. Pabba: I will find out tell sir
DURING THE FIRST 30 DAYS OF MY MEDICINE INTERNSHIP,
(1/10/2023 TO 31/10/2023)
I EMBRACED UNIT WORK, WHERE COORDINATION PLAYED A CRUCIAL ROLE, ENSURING TIMELY AND EFFECTIVE TREATMENT OUTCOMES FOR ADMITTED PATIENTS.
UNDER THE GUIDANCE OF MY MEDICINE HOD, I LEARNED TO MANAGE WORK EFFICIENTLY AND EXTRACT KNOWLEDGE FROM EVERY PATIENT SCENARIO. FROM IDENTIFYING CNS ABNORMALITIES BASED ON GAIT TO VITAL SKILLS, MY MEDICINE FACULTY PROVIDED EXCEPTIONAL GUIDANCE.
KEY LEARNING POINTS:
1. EFFECTIVE HISTORY TAKING
2. FORMULATING PROVISIONAL DIAGNOSES
3. INTERPRETING ECG AND CHEST X-RAYS
4. PERFORMING ECHO AND ULTRASOUND EXAMINATIONS
5. ADMINISTERING IM AND IV MEDICATIONS
6. MAINTAINING BP AND FEVER CHARTS
7. COMPREHENSIVE SYSTEM EXAMINATIONS
8. INSTRUCTING UNDERGRADUATE STUDENTS IN EXAMINATION TECHNIQUES
9. VITALS MONITORING AND PREDICTING PATIENT SEVERITY
10. EFFECTIVE COMMUNICATION WITH PATIENTS AND ATTENDANTS
11. UNDERSTANDING ENZYME MODIFICATIONS LINKED TO ORGAN PATHOLOGY
12. BASIC KNOWLEDGE OF NACO AND ICTC
13. STRATEGIES FOR TREATING STROKE PATIENTS
14. APPROACHES TO MANAGE HYPOTENSIVE PATIENTS
15. UNDERSTANDING THE LINK BETWEEN ALCOHOL AND DILATED CARDIOMYOPATHY
PERIPHERALS
MY PERIPHERALS ROTATION FROM NOVEMBER 1, 2023, TO NOVEMBER 15, 2023. THIS ROTATION ENCOMPASSES ICU, NEPHROLOGY, AND WARD DUTIES.
WITHIN THE ICU, I HAVE ENCOUNTERED CRITICALLY ILL PATIENTS, AND AT TIMES, I FELT OVERWHELMED BY THE GRAVITY OF THEIR CONDITIONS. INITIALLY, I DOUBTED MY EMOTIONAL STRENGTH AND CONSIDERED AVOIDING MY DREAM DEPARTMENT IN RESIDENCY. HOWEVER, MY HEAD OF DEPARTMENT (HOD) SUPPORTED, GUIDED, AND TAUGHT ME MANAGEMENT OPTIONS, INSTILLING CONFIDENCE IN DEALING WITH CRITICAL PATIENTS. I AM DEEPLY GRATEFUL TO MY FACULTY, POST-GRADUATE SUPERVISORS, AND MENTORS FOR THEIR UNWAVERING SUPPORT.
IN NEPHROLOGY, I LEARNED TO CONTROL AND MAINTAIN VITALS FOR HYPERTENSIVE PATIENTS UNDERGOING DIALYSIS. I GAINED INSIGHT INTO THE DIALYZER'S MECHANISM, PARTICULARLY OSMOSIS IN BLOOD PURIFICATION, GUIDED BY MY HOD.
MY LEARNING POINTS INCLUDE
1. CPR,
2. ABG SAMPLE COLLECTION AND INTERPRETATION, 3.FOLEY'S CATHETERIZATION,
4.RYLES TUBE INSERTION AND POSITION VERIFICATION,
5.ASCITIC TAP PROCEDURE,
6.ASSISTING AND SUTURING DURING CENTRAL LINE INSERTION,
7. MONITORING VENTILATED PATIENTS AND ADJUSTING SETTINGS,
8.MAINTAINING PATIENTS ON IONOTROPE SUPPORT, ADJUSTING INOTROPE DOSES,
9.MANAGING HIGH GRBS ON INSULIN INFUSION PUMP,
10.BED SORE DRESSING,
11.CONTROLLING BP IN DIALYSIS PATIENTS, AND 12.UNDERSTANDING DIALYSER SETTINGS LIKE UF RATE,
13.ALONG WITH 7-POINT GRBS MONITORING.






ASCITIC TAP PROCEDURE

MONITORING VITALS

INTERPRETATION OF 2D ECHO

VENTILATOR SETTINGS


Comments
Post a Comment